What 19,620 Public Comments Reveal About the July 1 Loan Changes
A look inside the voices behind the data — nurses, social workers, students, and faculty in their own words.
19,620 people wrote in. Most of them were scared of the same thing: who will care for patients if the people training to care for them cannot afford to finish their training?
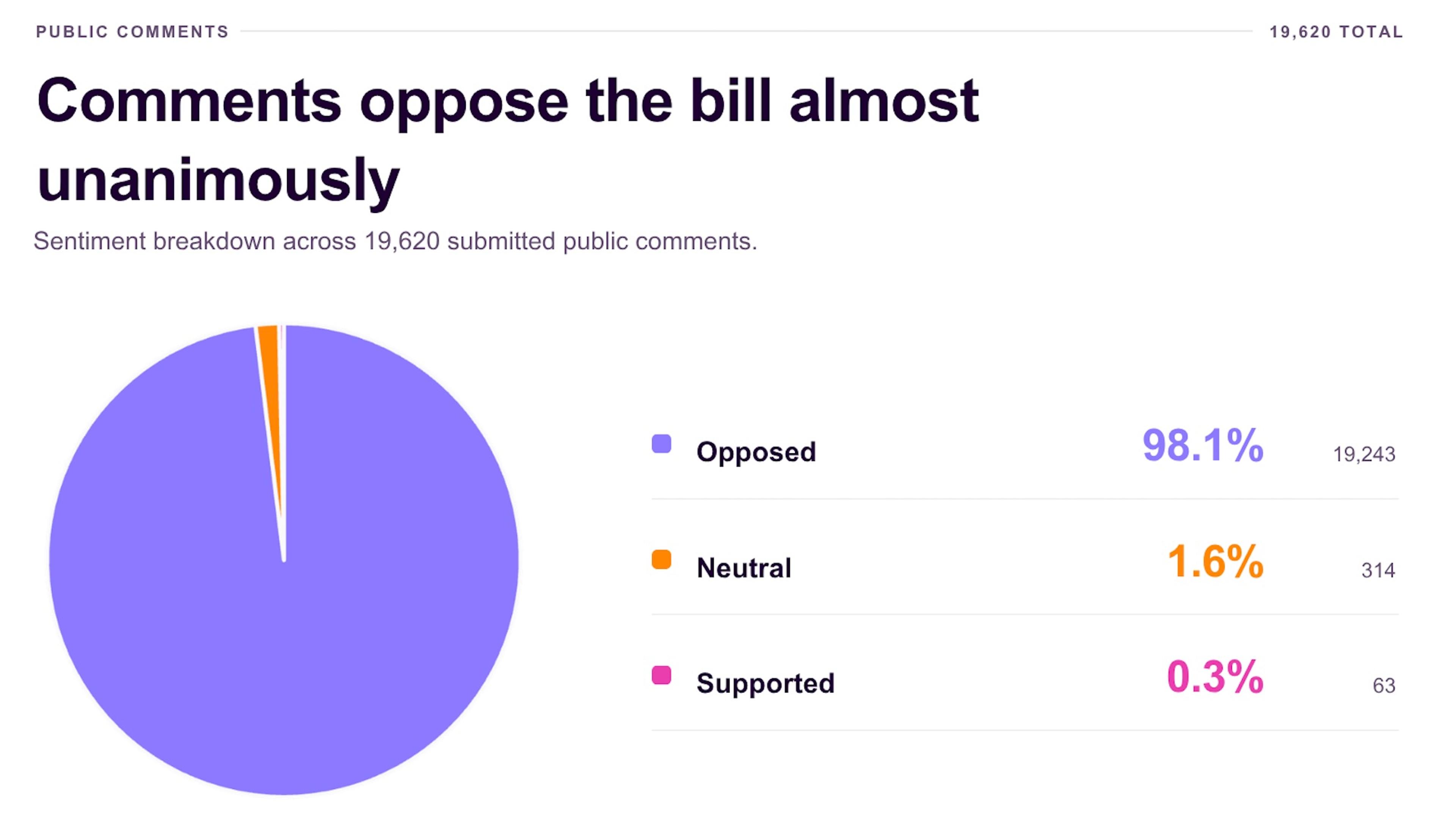
We analyzed all 19,620 unique public submissions posted to regulations.gov between January 30 and March 23, 2026. The numbers are striking on their own — 98.1% opposed the changes and only 0.30% supported — but they only tell part of the story. The comments themselves — many written by nurses on overnight shifts, social work students between clinical hours, and faculty watching their applicant pools shrink — say what no chart can.
This post details just a small sample of the comments submitted directly to the public record. Each was submitted to regulations.gov and is publicly viewable. We have shared them here exactly as they appeared.
“We are already short-staffed. This will make it worse.”
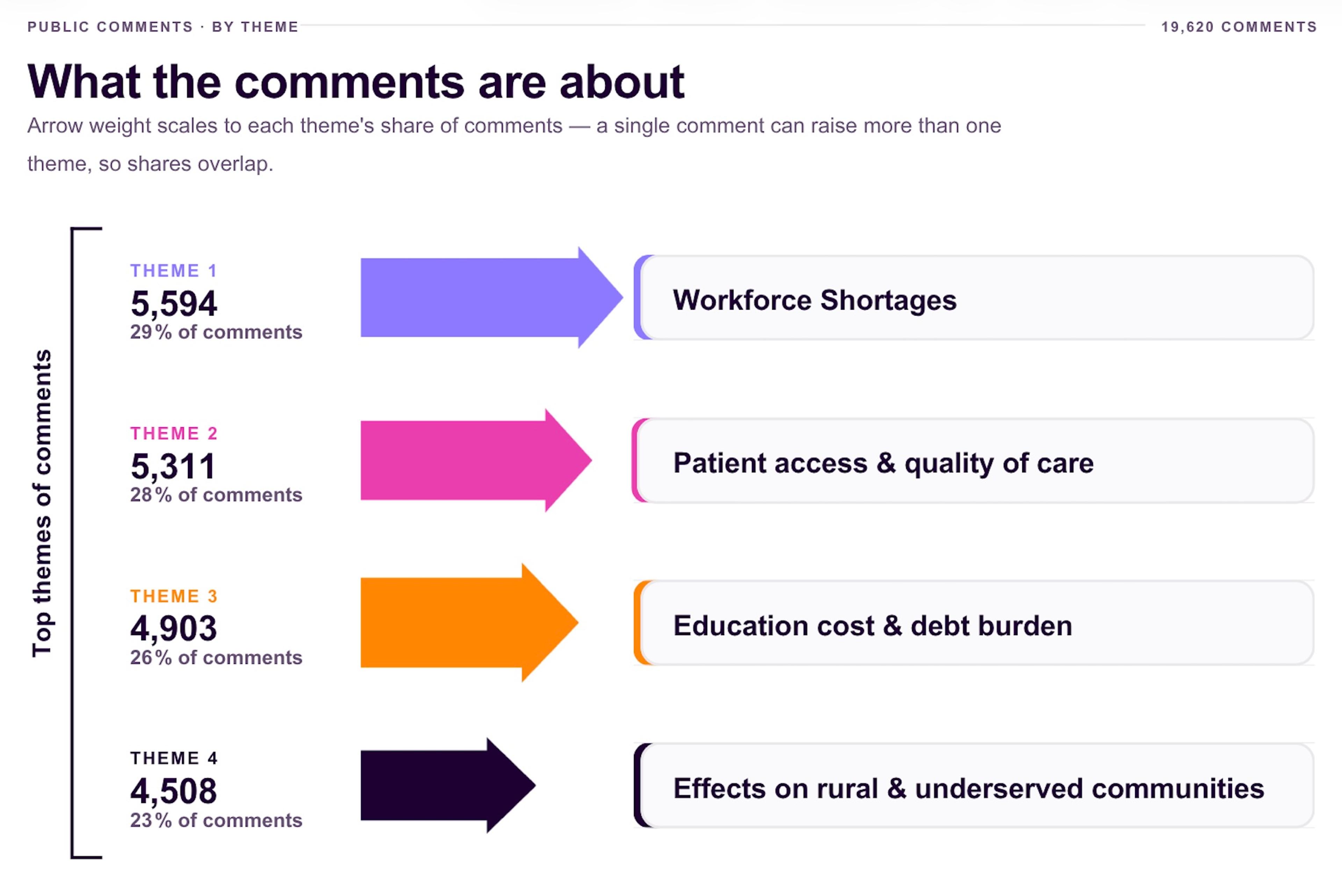
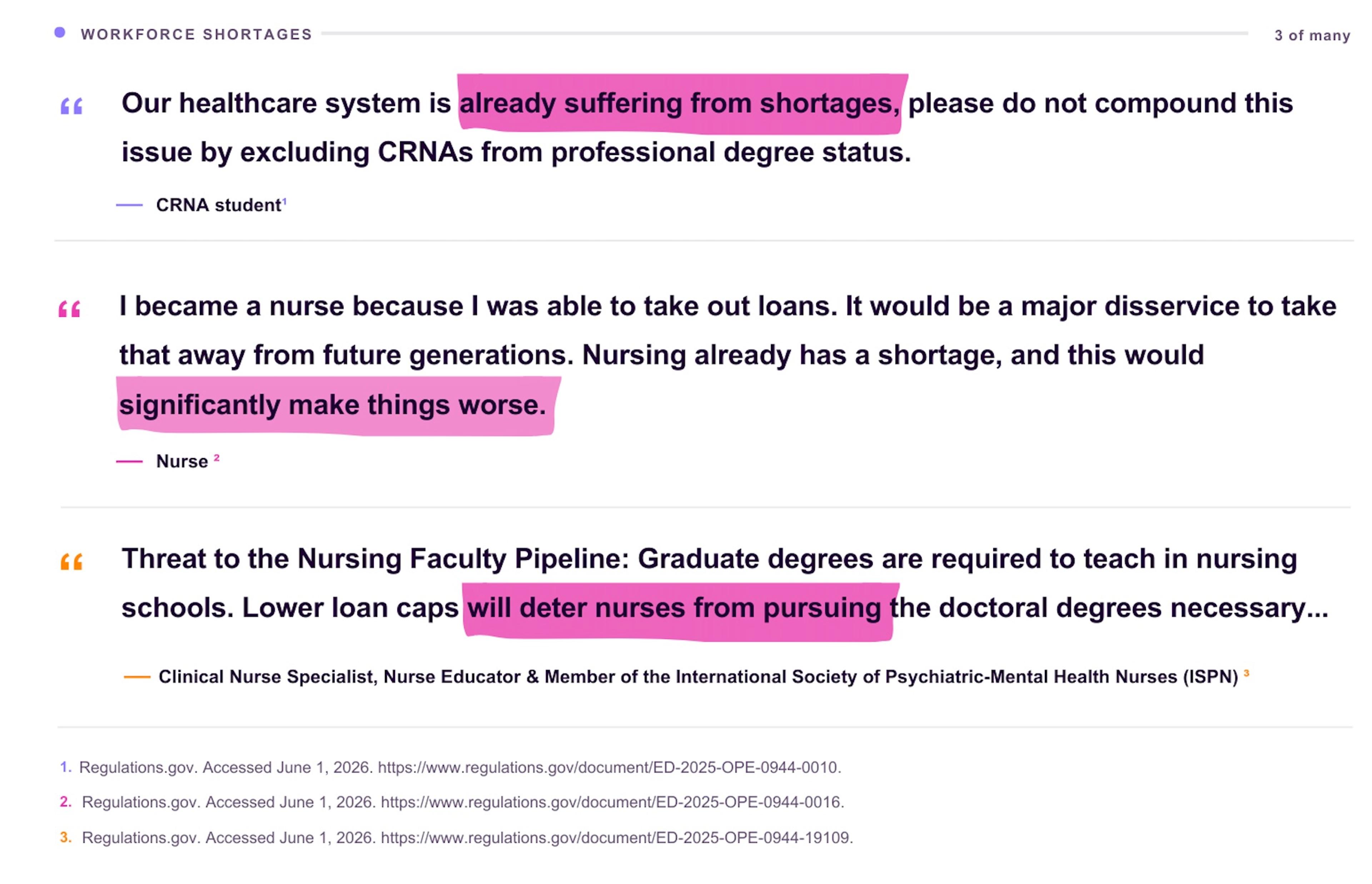
The most common theme across opposing comments was workforce shortages. Roughly 1 in 3 opposing submissions — 5,594 in total — raised concerns about healthcare staffing. Nurses described mandatory overtime and skipped breaks. Social workers described caseloads in the triple digits. Behavioral health providers described months-long waitlists for new patients.
The comments came from every state and nearly every clinical setting. A recurring thread: people who chose a healthcare career under one set of financial assumptions worry the next generation won’t get to make the same one.
“My patients will feel this before I do.”
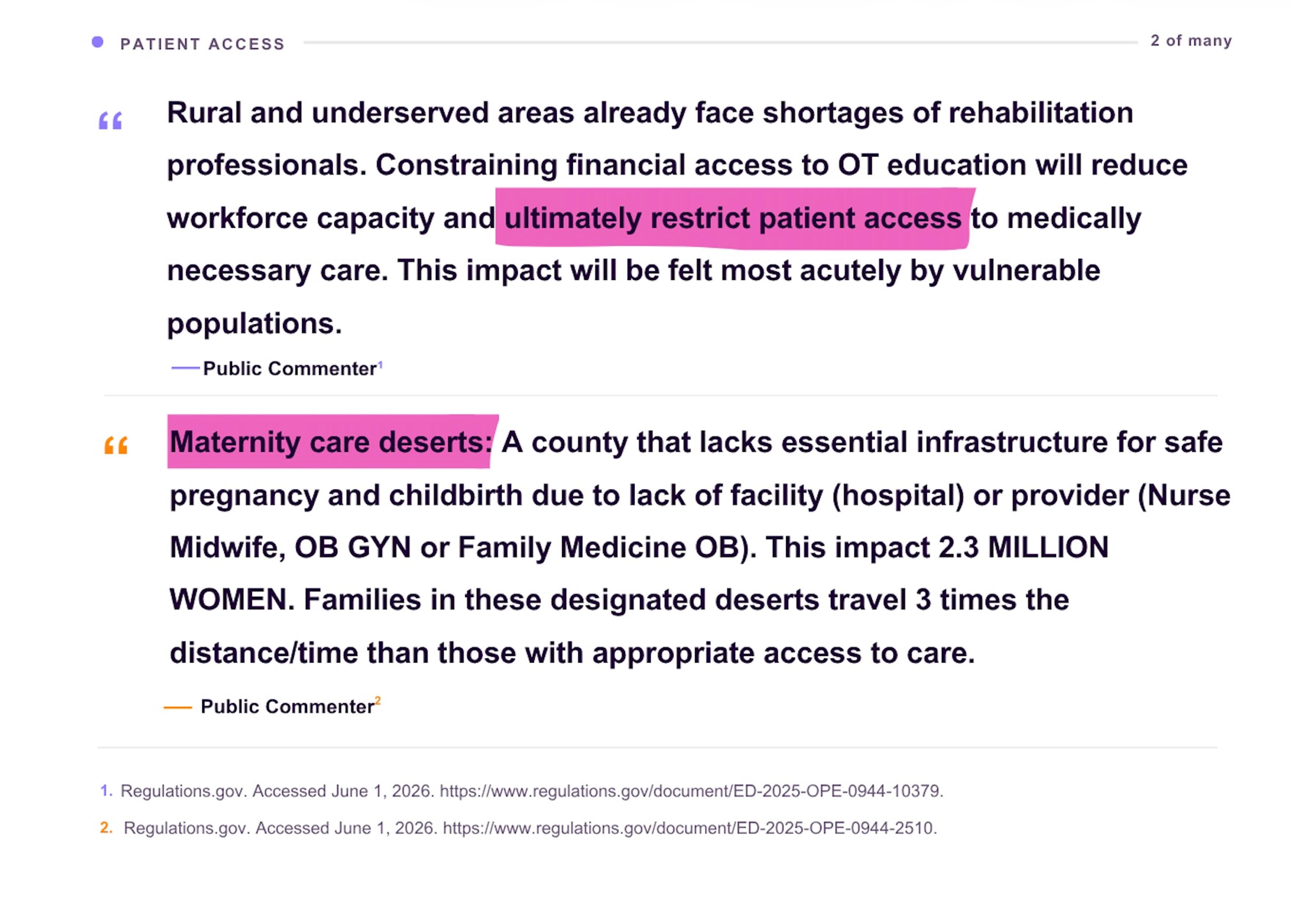
More than 1 in 4 opposing comments — 5,311 submissions — connected the borrowing changes to patient access. Commenters described patients who already drive an hour or more to reach a prenatal visit, a mental health appointment, or a physical therapy session. Fewer trained clinicians, they warned, means longer drives, longer waits, and some patients giving up on care entirely.
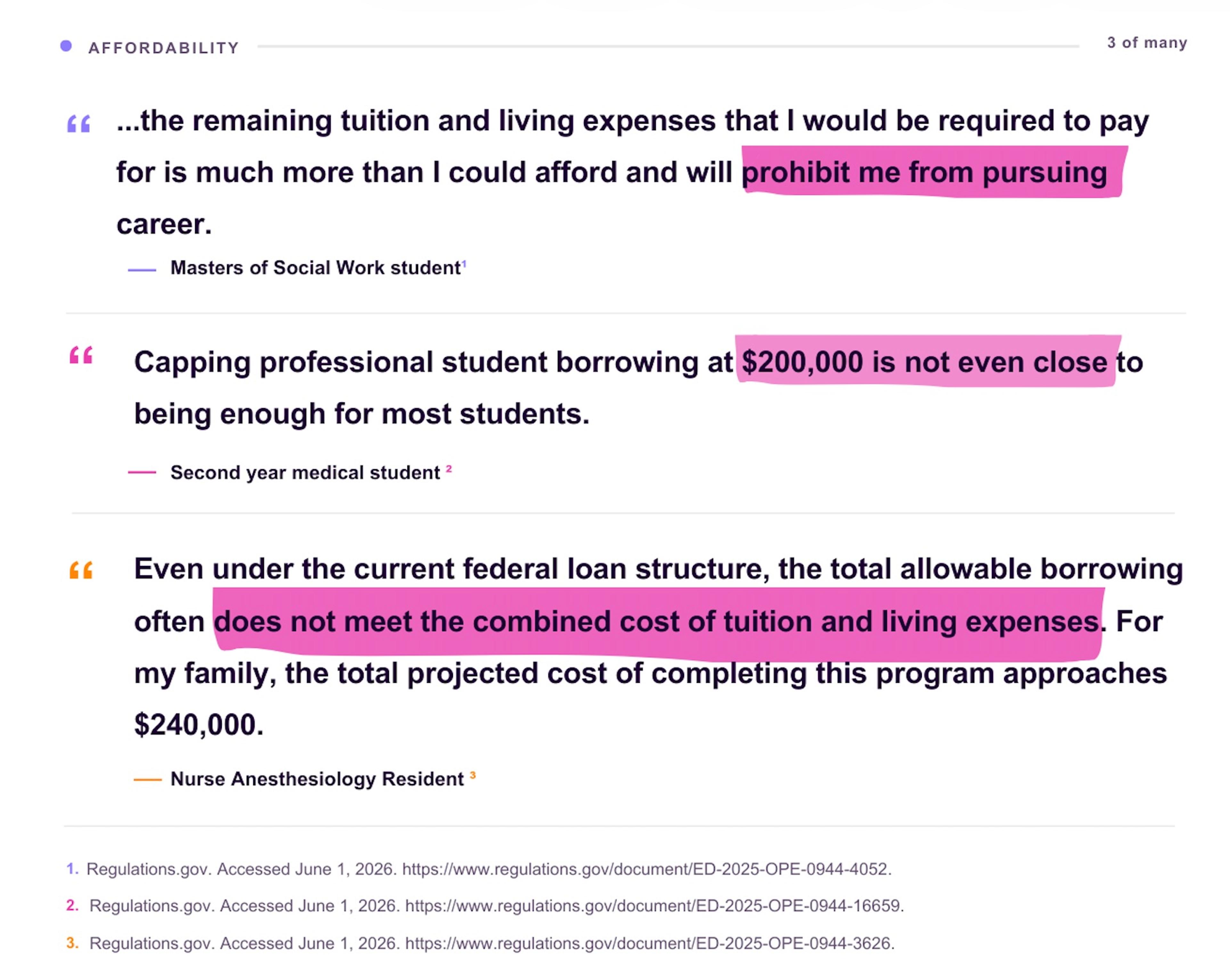
"I cannot do this without federal loans."
Affordability ran through 4,903 submissions, and concerns about borrowing limits specifically appeared in 5,232. The new framework caps annual graduate borrowing at $20,500 for programs that no longer qualify for the professional-degree designation. Commenters listed tuition figures that exceed the cap before accounting for housing, transportation, books, or clinical placement fees.
The tuition gap was not only described by individual commenters. The American Academy of Physician Associates reported median physician assistant program tuition of approximately $96,900, nearly five times the proposed annual cap, while Russell Sage College noted that nurse anesthesia tuition can reach $240,000 and warned of substantial funding gaps under the proposed cap structure.
Many commenters were prospective students still deciding whether to apply. Their comments often ended with the same line, phrased differently: "I do not know if I can do this."
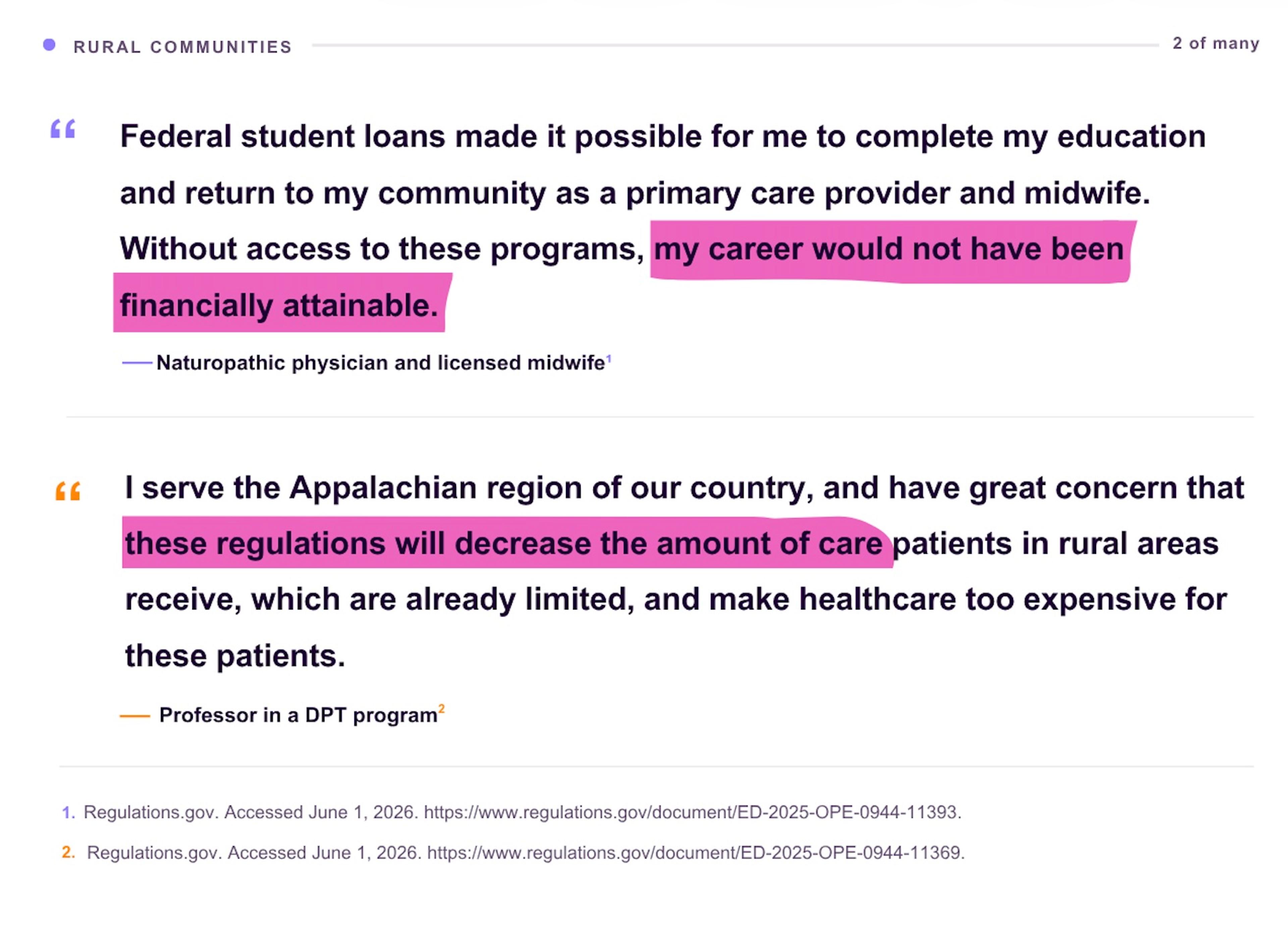
"If we leave, no one is coming to replace us."
4,508 comments came from rural and underserved communities, places that already lose the recruitment race, written by the people who came back anyway. Many came from clinicians who grew up in the towns they now serve and said federal loans were the only reason they could return. They described single-clinician clinics, county hospitals on the edge of closure, and patient panels that include people they have known since childhood.
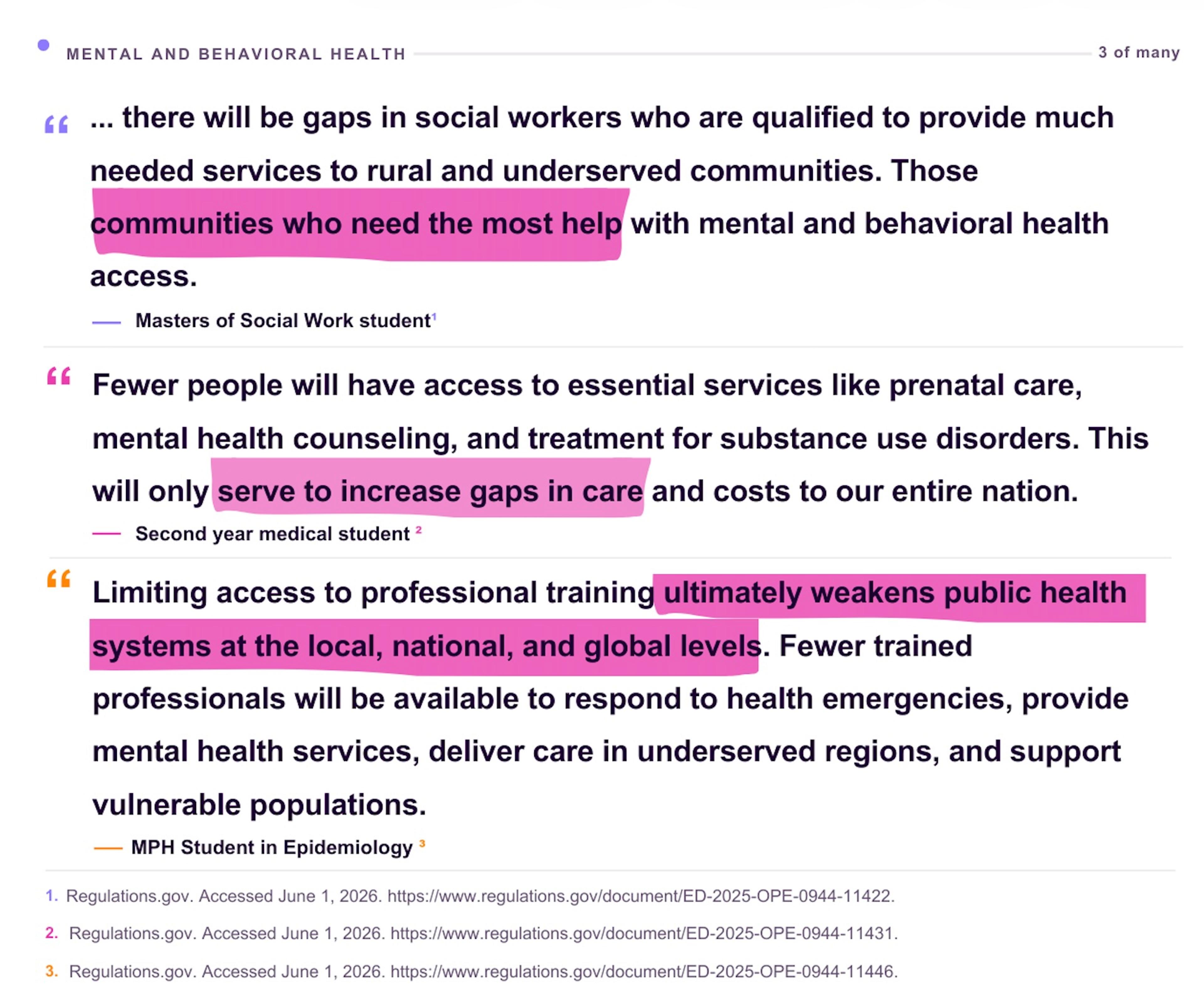
"We are the safety net that is already fraying."
Mental and behavioral health appeared in 3,117 submissions, and those comments carried the most urgency. Counselors, clinical social workers, psychologists, and marriage and family therapists described a workforce already stretched past capacity, serving patients in active crisis. The professions most affected by the borrowing changes are also the professions most relied on to meet rising demand for behavioral health services.
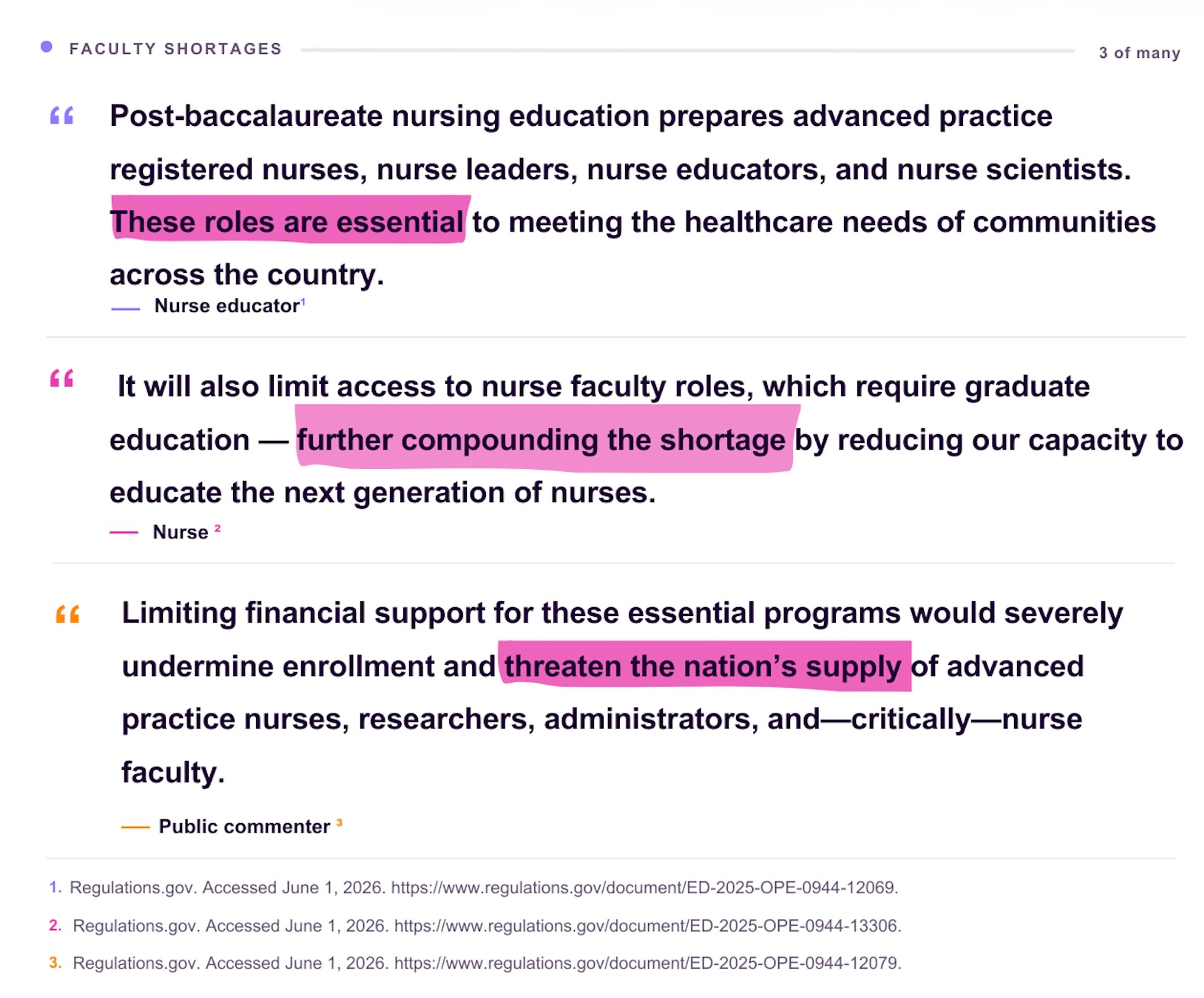
"If students cannot afford the degree, who will teach the next class?"
A theme we did not anticipate, but that appeared again and again: concerns regarding faculty shortages. Nursing school deans, physician assistant program directors, and therapy program chairs warned that the borrowing changes would not just reduce student enrollment. They would shrink the pool of future educators. Doctoral programs in nursing, the pipeline for nursing faculty, are among the programs no longer qualifying for the higher borrowing limits.
Comments from individual faculty members echoed the same concern.
Professional associations and academic institutions raised the same concerns

Alongside the tens of thousands of individual comments, the docket included formal submissions from professional associations, universities, and academic institutions. These letters carried the weight of organizational data: enrollment projections, applicant trends, tuition benchmarks, and program-level analysis, and their conclusions tracked closely with what individual commenters described in their own words.
Johns Hopkins University submitted enrollment modeling projecting a 25% decline in nursing master's enrollment and a 15% decline in doctoral nursing enrollment under the new borrowing framework. The university also highlighted an equity dimension that runs through much of the dataset: 53% of affected Grad PLUS borrowers are Pell-eligible, meaning the borrowers most likely to lose access are those who came to graduate study from lower-income undergraduate backgrounds.
The American Association of Colleges of Nursing (AACN) reported that 78% of nursing school deans believe the changes would negatively affect enrollment, and 77% believe they would damage the future faculty pipeline, a finding that directly mirrors the faculty-worry theme that appeared throughout individual comments. Doctoral nursing programs, the pipeline for the next generation of nursing faculty, sit squarely among programs no longer qualifying for the higher borrowing limits.
The American Occupational Therapy Association (AOTA) noted that occupational therapy applications have already declined 33% since 2018, before the borrowing changes take effect. AOTA's analysis also found that only approximately 29 of more than 322 occupational therapy programs fall below the proposed $20,500 annual borrowing limit. For the overwhelming majority of accredited OT programs, federal loans alone would not cover this gap.
The American Academy of Physician Associates (AAPA) reported median physician assistant program tuition of approximately $96,900, and Russell Sage College documented nurse anesthesia tuition reaching $240,000, with both institutions warning of substantial funding gaps under the proposed cap structure. Where individual commenters cited tuition figures from their own programs, the association data confirmed those figures are not outliers; they are the median.
Taken together, the formal association and institutional submissions did not contradict the individual comments. They quantified them.
Concerns that extend well beyond nursing
Public attention has focused heavily on nursing, and for good reason, but the comments themselves reflected a much broader group of professions. Social workers, physician assistants, occupational therapists, physical therapists, speech-language pathologists, mental health counselors, marriage and family therapists, nurse anesthetists, and nurse midwives all appeared frequently throughout the dataset.
Many commenters explicitly framed the issue as a healthcare workforce question rather than a nursing question. They pointed out that patients rarely encounter a single profession in isolation. A hospital stay might involve a physician, a nurse, a physical therapist, a social worker, a pharmacist, and a respiratory therapist, all in a single day. Restricting borrowing for some of those professions while preserving it for others, commenters argued, would reshape who enters the care team.
What healthcare employers are doing in response
Healthcare employers are not waiting for the policy debate to resolve. Across the country, hospitals and health systems are expanding loan repayment programs, tuition assistance, and employer-sponsored financing to recruit and retain clinicians in hard-to-fill roles. For employers already facing shortages in nursing, behavioral health, therapy, and advanced practice, these programs have moved from perk to core strategy.
At Clasp, we work with healthcare employers to tie student loan repayment to long-term employment, helping organizations attract clinicians earlier in their training and improve retention once they arrive. The comments analyzed here reinforce something employers have been telling us for years: the financial path into clinical work is one of the most powerful levers available for shaping the future workforce.
The story behind many of the comments in this docket is one financial aid offices know well: a qualified, admitted student maxes out federal aid, applies for a private loan, is declined for lack of a co-signer, and stops out, sometimes weeks into a program they have already started. Under the new $20,500 annual cap, that sequence will play out for a much larger share of healthcare graduate students, and far earlier in their training. The pipeline does not break because students give up on the profession. It breaks because the financial aid system runs out of options before the student does.
Clasp gives institutions a path forward for those students. We work with universities to stand up institutional lending programs – loans the school itself offers to its own students to bridge the gap between federal aid and the actual cost of attendance. The goal: a qualified borrower who cannot secure a private loan without a co-signer has a path that keeps them enrolled. The university holds the credit risk and sets the policy. Clasp does everything else: the digital application experience the student sees, the compliance overlay that keeps the program inside regulatory lines, the people who interact with students through underwriting and disbursement, and the tools that let the financial aid team coach borrowers and manage the program. For schools whose programs are now most exposed to the borrowing changes, an institutional loan program is one of the few levers that help keep an admitted, motivated student enrolled rather than stopping out.
Methodology
This analysis covers the 19,620 public submissions filed to regulations.gov related to federal graduate borrowing changes between January 30 and March 23, 2026. The dataset included 17,844 text-based comments and 1,776 attached documents and formal letters, each reviewed individually as part of the broader analysis. The 1,776 attached submissions are a subset of the 19,620 total, not an additive figure. All submissions were retrieved directly from the docket’s public record.
Many submissions were filed not as typed text but as scanned PDFs, photographs of letters, or image attachments. To make these analyzable, attached documents were processed with pdfplumber to extract machine-readable text. Documents that failed extraction or returned low-confidence output were flagged and reviewed by hand. Submissions consisting solely of images with no extractable text, such as photographs without captions, were kept in the corpus but classified as neutral unless a reviewer assigned a position.
Each submission was then classified along four dimensions (profession mention, theme, geography, and stance) using an in-house rule-and-keyword classifier. The script assigned a stance of oppose, support, or neutral and extracted profession, theme, and geography by matching submissions against defined keyword and pattern sets. Explicit oppose and support labels were reserved for comments using clear, unambiguous language. Neutral submissions were primarily personal stories, patient experiences, photographs, or comments that did not state a clear position.
To check that the classifier applied these definitions consistently, a random sample of 25 submissions was hand-labeled by a reviewer and compared against the script’s output, with disagreements resolved in favor of the neutral category. Theme percentages are calculated as a share of the 19,243 opposing submissions, and individual submissions may reflect more than one theme, so a single comment can count toward multiple themes.
Large coordinated form-letter campaigns are common on dockets of this size and can inflate raw counts. To avoid this, near-identical form letters were collapsed into representative entries rather than counted individually.
Statistics and projections attributed to formal association and institutional submissions, including Johns Hopkins University, the American Association of Colleges of Nursing, the American Occupational Therapy Association, the American Academy of Physician Associates, and Russell Sage College, were drawn directly from the comment letters and supporting documents those organizations posted to regulations.gov during the comment period.
The screenshots in this post were selected from a larger pool of comments addressing the same theme, chosen to present the clearest example of each. Personally identifying information has been redacted, though the original comments remain publicly accessible on regulations.gov.
Reading the comments in full
The full public docket remains available on regulations.gov. We encourage anyone working in healthcare policy, education, or workforce planning to read the comments directly.
Learn more about how Clasp partners with healthcare employers to strengthen clinical workforce pipelines through loan-linked hiring.Learn more about how Clasp partners with schools to help students with gap financing through an institutional lending program.